Deep brain stimulation: An effective but poorly understood treatment
Deep brain stimulation (DBS) has grown in popularity over the past 15 years as a treatment for movement-related neurological disorders and a potential treatment for other neurological disorders. What was a serendipitous discovery during target localization for a lesioning procedure has turned into a widely-used effective method to suppress pathologic tremor and certain disease symptoms. DBS is currently an approved medical treatment for Parkinson’s disease (PD) and essential tremor (ET) patients. It involves the placement of an electrode in a region of the brain that has been discovered to be associated with generating pathologic symptoms, namely the basal ganglia (BG) in the case of these motor disorders, and programming the implantable pulse generator (IPG) with appropriate stimulus parameters, such as the amplitude, pulse width, and frequency of the continuous current pulse trains delivered to that target.
Parkinson’s disease is associated with the loss of dopaminergic cells in the substantia nigra (SN) nucleus of the BG and causes patients to exhibit resting tremor, bradykinesia, rigidity, postural instability, depression, and cognitive impairment, all of which are disabling and detrimental to the patients’ quality of life[1]. While DBS has demonstrated great success in suppressing tremor and relieving other motor symptoms, its benefits vary widely between patients, and cognitive and psychiatric impairment as well as parasthesia and disorientation can result [2]. The main decisions that need to be made in administering DBS therapy are target location and stimulus parameter settings, and have generally been determined empirically [3, 4]. These trial-and-error approaches have been necessitated out of the lack of understanding of DBS's efficacy. Hypotheses on the mechanism of DBS range from inhibitory mechanisms to excitatory mechanisms and information lesions [13, 33, 37]. General practices of parameter settings seem to converge on frequency settings in the 120-185Hz range, pulse widths in the 50-75s range, and amplitudes between 2-3.5V [13, 33, 37]. However, a systematic approach to setting parameters has not been found and leaves physicians little confidence as to the most appropriate settings and electrode configuration for the patient. Side effects and discomfort are most commonly corrected by an adjustment of settings, requiring a visit to the doctor [10].
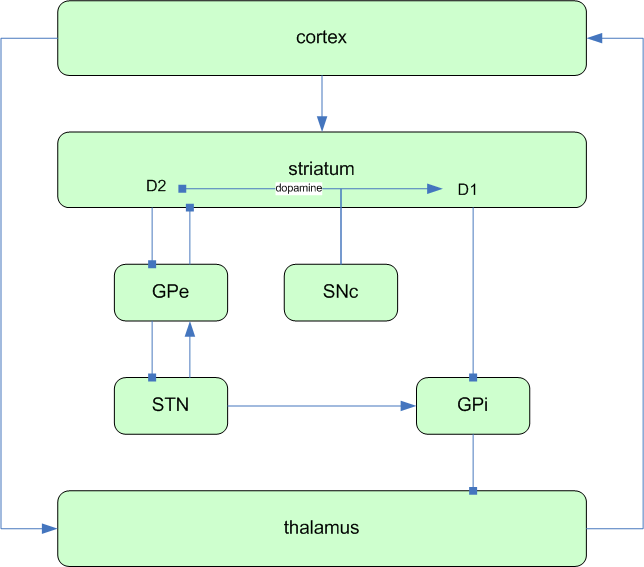
A couple groups have studied the clinical effect of various settings for DBS in Parkinson’s [4] and essential tremor patients [11]. However, only a coarse relationship has been defined, namely that frequencies above 100Hz are most effective, and has been derived from studying the effect of single parameters treated as independent variables on clinical outcome. Additionally, these groups suggested a general optimal setting, presumably for any patient at all times. The complexity of the basal ganglia circuitry may prevent a complete explanation of the mechanism of DBS any time soon (see Fig. 2). Nevertheless, the specific and time-varying needs of patients require adaptive DBS control which relate the empirically determined clinical effects to the underlying electrophysiological changes.
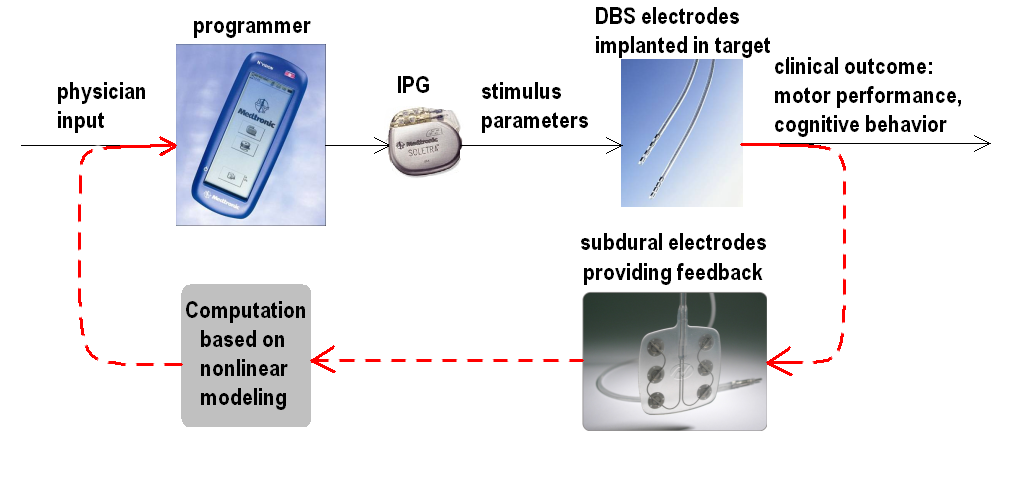
Figure 1) Concept diagram of a closed-loop DBS system: Current DBS systems deliver electrical stimulus to the targeted region of the brain without taking into account the changes it induces in the patient’s symptoms; i.e., DBS is delivered blindly because there is no feedback to the system regarding the patient’s current and needs for stimulation. By adjusting stimulus parameters based on continuously monitored neural correlates of the patient’s symptomatic state, the closed-loop DBS system provides therapy which targets the patient’s specific and changing needs. The type and location of feedback electrodes and computational algorithm to be used will be determined during the course of this research.
Main Objective: Closing the loop for adaptive control of motor and psychiatric effects
The long-term goal of an adaptive closed-loop system is depicted in Figure 1.
In broad terms, my long-term objective is to improve the clinical benefit of DBS in Parkinson’s patients while minimizing psychiatric changes and complications. My primary research goal will be to develop a closed-loop DBS system which will continuously monitor the status of DBS effects and adjust parameters according to the patient's moment-by-moment needs. To accomplish that goal, I will focus on the following objectives on the road to the ultimate evaluation of the closed-loop DBS system in clinical trials.
Localize the major areas that are affected and which form neural correlates of DBS effects, categorized as motor and psychiatric/cognitive effects, by measuring global activation maps.
Develop a method for continuously monitoring the electrical activity in the neural correlates determined in (1) simultaneously with measurements of clinical motor and psychiatric outcome while varying stimulus parameters.
Determine the relationship between neurophysiological changes and the clinical outcome of motor performance and cognitive and psychiatric behavior.
Determine the relationship between stimulus parameter settings with the monitored neurophysiological changes.
Develop an algorithm based on the results of (3) and (4) to adjust stimulus parameters based on the status of continuously monitored signals for optimizing motor and psychiatric effects simultaneously.
Measure the effects of DBS on neural plasticity and determine whether it can be modulated to produce longer-lasting and more beneficial effects.
In particular, the closed-loop system will be developed to treat PD by monitoring the pathophysiological effects of the degenerating BG. I will conduct research to determine the following: what electrophysiological signal to use as feedback; the mode of acquiring and monitoring this signal; the representation of information in these neural signals regarding the motor and cognitive state; and a model of the transformation from the delivered stimulus to the affected neural activity in order to implement a computational algorithm for translating the monitored neural signals into desired stimulus parameters. All of this work will ideally be carried out in human patient subjects. Such studies are feasible at USC due to the available collaborations and funding opportunities described in the last section.
Localization of neural correlates through global spatial activation patterns
The first problem to tackle is to locate the neural ensembles that are most sensitive to changes in DBS parameters and will provide the most information about the motor and psychiatric effects of DBS. Electrophysiological studies have identified feedback and reciprocal pathways involving the BG which provide possible mechanisms by which degeneration of BG neurons in PD could cause motor and cognitive disabilities, and furthermore, indicate areas that would provide the relevant feedback information for a closed-loop DBS system [12, 13] (see Fig. 2). Electrophysiological microelectrode recordings have been performed during DBS to determine how stimulating the subthalamic nucleus (STN), for instance, changes the firing activity of efferent targets. However, results have been conflicting [13, 33, 37], and the only measurements extracted from those recordings have been those of average firing rates. To measure average activity, alternative methods, such as positron emission tomography (PET), exist which have do not have near the procedural complexity or invasiveness of microelectrode recording; furthermore, PET imaging can acquire measures of average activity more globally across the brain in a non-invasive efficient manner and is already approved for use on humans. Rather than measuring electrical activity directly in local populations at higher precision, PET imaging provides a global picture of the anatomical areas most affected by DBS through measures of regional cerebral blood flow (rCBF) or regional cerebral metabolic rate of glucose (rCMRGlc) which present [13, 33, 37]. MRI would provide higher temporal resolution, but cannot be used on patients with implanted DBS devices.
Imaging studies can provide spatial activation maps that reveal which neural areas are affected by DBS and to what degree. Analysis of DBS effects can then be focused on the area(s) implicated as regions of interest. A number of studies have been performed to measure rCBF and rCMRGlc, which indicates the level of oxygen and glucose metabolism caused by synaptic activity, in Parkinson’s patients with DBS [13, 33, 37]. However, these studies were conducted for the purpose of determining which areas were affected by stimulation of STN, but none to date have measured how changing DBS stimulus parameters affects spatial activation nor have they focused on localizing neural correlates of cognitive effects. While psychiatric side effects have been noted as generally mild and transient, they still contribute to the patient’s overall experience and comfort with DBS, and in some cases have been detrimental to a patient's family and personal life [13, 33, 37]. Thus far, solutions to cognitive or mood impairment have primarily included management of expectations and education of patients and caregivers or selection of patients who have no previous history of psychiatric disorders [22, 23]. While these subjective approaches may be helpful, I believe an investigation of the neurophysiological effects of DBS and how these neurophysiologic changes lead to improved clinical measures will reveal how DBS can be engineered to provide symptomatic relief with minimized side effects. With a clearer understanding of its mechanisms, DBS can be developed more efficiently for improved treatment of current indications and treatment of new indications.
PET imaging could be used to initially localize neural correlates and later to assess the long-term effects of optimizing stimulation parameters. The major limitation of such a study would be the duration required to scan the patient at various parameter settings. Separate scans could be taken with parameters set to extremes, so that the areas can be identified which show the most correlated changes in activity with changes in parameters. Careful planning will allow efficient acquisition of enough points to perform statistical analysis. PET imaging studies in PD patients are already conducted at the PET Imaging Center at USC, directed by Dr. Pete Conti. To perform the desired study of mapping neural activation at various parameter settings, FDG, already used at USC, or H2150 can be used. Drs. Giselle Petzinger and Mark Liker’s PD patients form a readily available subject pool from USC’s Neurology and Neurosurgery Departments.
Monitoring neural correlates of pathology and measuring clinical outcome
Depending on which areas are implicated, appropriate methods of acquiring signals from these areas will be developed and appropriate clinical measures must be chosen. Implementation of the closed-loop system will require chronic monitoring capabilities in the indicated areas. During development phases of the optimization algorithm, clinically relevant outcomes must also be simultaneously measured.
One key challenge will be to develop a way to chronically and continuously monitor spatio-temporally varying spike activity in subcortical structures if the principal neural correlates of motor symptoms or psychiatric effects are localized in the more inferior brain structures. The STN sends synaptic projections to the anterior cingulate gyrus and neighboring areas in the prefrontal cortex, areas implicated in cognitive behavior [26, 27]. A limited number of results have shown that stimulation of STN causes significant increases in these regions. Hence, stimulation of STN may influence cognition and behavior through the existing anatomical infrastructure. Haeglen et al reported no changes in frontal limbic area activation, but this may be why the selected patients did not exhibit cognitive deficit [18]. The question is how varying the stimulation parameters affects patients psychiatrically and cognitively, and how these effects are correlated to changes in activation of the anatomical regions believed to be related to cognition and psychiatry. Although one group has implicated that electrode placement and stimulation parameters are possible factors in the appearance of cognitive changes, no study has been conducted yet to show how changes in these factors control cognitive effects [28]. Further studies, including a retrospective study of DBS patients who have experienced worsening cognitive and psychiatric behavior, are needed to confirm whether stimulation of STN excites limbic connections; determine the dependency of limbic excitation on stimulus parameters; and determine the relationship between the electrophysiological changes and clinical measures of mood and cognition, such as the Bisyllabic Word Repetition Test, Mattis Dementia Rating Scale, and Beck Depression Inventory scores [13, 33, 37].
STN and GPi signals can be monitored via DBS macroelectrodes [30]. However, such recordings can currently be done only in the short interval after surgical implant of the DBS leads and before the implantation of the IPG. A new type of DBS leads must be designed and manufactured which have both recording and stimulation capabilities even while connected to the IPG. Simultaneous stimulation and recording will poise noise and cross-contamination issues that will require careful design to resolve.
A possible location for the targeted motor correlate is the pre-motor cortex, which has been found in PET studies to be correlated to the motor improvements induced by DBS in the STN [20] (see Fig. 2). The dynamics in affected areas can be captured at a finer spatial resolution by epidural recordings for cortical areas and depth electrodes for subcortical structures. There are several advantages of epidural electrodes over various penetrating recording techniques. Epidural recording does not require crossing the blood-brain barrier and has been performed without any of the adverse hemorrhaging events that occasionally occur in invasive procedures, such as micro-electrode recordings [31]. It does not acquire signals with as much spatial precision as microwire or ceramic electrode recordings but population activity is still acquired with much more resolution than scalp EEG, for instance. Several contacts can be contained on a single strip or array in various configurations and locations. Although UDPRS-III scores are well-accepted and widely used measures for motor performance in PD patients, they are not readily measured on as short a time scale as would be needed to find correlations as the stimulus parameters are being changed with short time intervals. Therefore, we would more likely use accelerometers to measure tremor and reaction time tasks to evaluate bradykinesia, and develop an apparatus which can quantify rigidity, tremor, and bradykinesia during intra-operative and post-operative testing. One candidate design is a torque-based apparatus invented at Johns Hopkins which quantifies these parkinsonian characteristics based on analysis of viscoelastic biomechanics [32]. Rigidity may be measured with standard UDPRS evaluation; however, a torque motor apparatus would allow rigidity and bradykinesia measurements while stimulus parameters are changed relatively quickly [32]. The apparatus applies mechanical perturbations parameterized by the angular displacement, �(t), and measures the total torque, t (t), applied by the patient. The stiffness K and viscosity B of the flexor and extensor muscle groups as a whole and the overall inertia J of the hand can
then be determined according to Eq. 1:
t (t) = K�(t) + B�˙(t) + J��(t) + qoff (1)
where qoff is the offset torque. Bradykinesia will be assessed by the conventional means of reaction time and movement speed during a modified hand-tapping test.
Figure 2) A model of the connectivity between basal ganglia structures with one another and other regions heavily involved with motor control and cognition and mood. Arrows indicate excitatory input; circles indicate inhibitory input. ACG = anterior cingulated gyrus; PMd = dorsal premotor cortex; M1 = primary motor cortex; STN = subthalamic nucleus; GPe = globus pallidus externa; GPi = globus pallidus interna; SNc = substantia nigra pars compacta. Based on many previous studies, including [13, 33, 37].
Quantifying the dependency of clinical outcome on neural population activity
From data collected by means of the signal acquisition methods developed in the earlier stages of the research, the correlation between the neural activity and the clinical motor and psychiatric outcome must be identified. State-of-the-art nonlinear modeling methods developed at USC by Profs. Ted Berger and Vasilis Marmarelis will be adapted and applied to the problem of optimizing DBS stimulation parameters in order to extract a robust mathematical representation of the input-output transformation from continuously valued multi-variable neural correlates to the discrete-valued clinical measures of motor performance, mood, and cognition. The clinical outcome of the closed-loop system can be assessed and related back to measured neurophysiological changes.
Oscillatory local field potentials (LFP) have been observed and connected to motor execution [13, 33, 37]. Through such studies, associations between basal ganglia LFPs in different frequency bands and aspects of movement have been deduced: alpha rhythms (7-10Hz) to pathologic tremor; beta rhythms (11-30 Hz) pathologic activity related to movement initiation and inversely related to movement preparation; and gamma rhythms (> 70Hz) to a non-resting state.
The relationship between frequency spectra (see Fig. 3) of the regional neural activity and the clinical measures will be determined. For example, if only tremor was to be suppressed, it is possible that the single clinical measure may be correlated to the alpha rhythm independent of other frequency bands in which case only a first order filter would be necessary. However, spatiotemporal spectral patterns are expected to be found in which
Figure 3) A hypothetical example of the normalized power spectrum of fabricated data to help visualize a potential neural correlate multi-variable output which can be modeled by a nonlinear transformation of input stimulus parameters. Each LFP acquired from a different electrode may carry frequency-dependent information. The axis labeled “Channel #”, then, represents a spatial dimension. Interactions between frequency components in different locations can be captured in higher-order Volterra-Wiener kernels.
combinations of behavior in multiple frequency bands, requiring higher order filters to represent the transformation between the feedback neural activity and clinical output. Once the spatiotemporal spectra are mapped to different behavioral states, the adjustment of parameters to achieve the desired state-dependent spectral patterns will be determined. Phase differences across different recording sites may carry information?
Quantifying the dependency of neural population activity on changing stimulus settings
Once the changes in motor and cognitive state have been related to changes in the neural correlate, the next step is to define the input-output transformation from the stimulus parameter space to the neural correlate space. Closed-loop neural stimulation is not a novel concept; however, endeavors to design and implement a closed-loop DBS system have only begun recently [39]. Feng et al outline a computational algorithm that could potentially identify optimal DBS stimulus parameters; however, the algorithm has only been tested on simulated data and the authors themselves recognize “the incompleteness of the model.” Modeling studies can be helpful, but the complexity of the basal ganglia circuitry and its role in Parkinson’s disease prevents acceptance of any hypothetical algorithm until tested on human data. My current involvement with USC’s neurosurgeons and neurologists pave the path for translation of such optimization algorithms to clinical studies. This study also did not address the problem of designating bipolar or monopolar electrode configuration and which electrode(s) to use.
Furthermore, I would like to develop algorithms based on our knowledge and understanding of the basal ganglia network. Extensive research on anatomical connections has revealed feedforward and feedback connections between the thalamus, frontal cortex, and basal ganglia [13, 33, 37]. Even while the understanding of the underlying pathophysiology to parkinsonian symptoms is incomplete, the algorithms developed for this closed-loop DBS system should be consistent with the underlying physiology of basal ganglia circuitry and connections with cortical and thalamic regions. The closed-loop system should be developed and evaluated in light of current physiological network models and checked for new insight into these networks. For example, one model that is supported by anatomical and electrophysiological evidence is shown in Fig. 2. Suppose parkinsonian tremor occurs because SNc is not regulating striatal output as it should, and synchronous oscillatory discharge is the normal resting (akinetic) state, but since the cortex is not driving the striatum in the absence of intended motor execution, the oscillatory circuits take over. In this case, the desired effect of DBS is to inhibit or mask the oscillatory output originating in GPi or STN. At the same time, we will be concerned about how this affects thalamic feedback paths to the cortex because that could influence the limbic system and cognitive areas in the frontal cortex.
Finding an optimal setting requires an analytical tool that can deal with a large parameter space and determine interdependent dynamic relationships between all the parameters and the clinical outcome. Handling a large parameter space practically requires efficient methods. With the current precision and range of parameter values available through the programmer, the programmer is already capable of thousands of settings, but complexity will only increase as features are enhanced or expanded by adding more electrodes, for example. Some choices, such as electrode spacing, and the extent of some features, such as the 0-10V range of stimulus amplitudes, are available but not exploited because of the inability to predict the clinical effect or the impracticality of a physician attempting every setting and choosing the ‘best’ one. A computational algorithm that analytically determines the appropriate combination of electrode configuration, amplitude, and frequency as an interdependent parameter set allows automated control designed for optimized settings.
Clinical results already indicates that while increasing frequency and amplitude increasingly suppress tremor, increasing voltages increase side effects and increasing frequencies decrease the therapeutic window, defined as the range of voltages for which tremor suppression was maximized and side effects were deemed tolerable (cite Kuncel 06). The algorithms developed will quantitatively determine the settings that will allow an optimal tradeoff between suppression of motor symptoms and minimization of sensational and cognitive side effects.
Drs. Ted Berger and Vasilis Marmarelis have developed nonlinear modelling methods which efficiently extract spatio-temporal relationships between input spike trains and output spike trains [40, 41]. The input-output transformations are represented by a series of Volterra kernels that contribute to the output for various combinations of input spike occurrence times. Now, a method needs to be developed to which can similarly identify the relationship not between Poisson spike trains, but between relevant features of the neural population activity and the patient’s motor and psychiatric behavior. Rather than determining how the occurrence of an output spike depends upon the occurrences and co-occurrences of input spikes that form a temporal input spike pattern, the motor and psychiatric test scores will need to be related to combinations of continuous neural activity on the multiple channels. At the same time, the mathematical representation of the dependency between characteristics of neural activity and the stimulus parameters will drive DBS control. The former model provides information about the desired change in motor and psychiatric output affected through changes in neural activity while the latter model informs the system on how adjustment of parameters will affect the neural state, so that the patient symptoms can be treated reliably and optimally.
Modulating neuroplasticity through DBS
DBS may cause long-term changes in the neural substrate but the interaction between DBS and neuroplasticity in Parkinson’s patients is yet to be studied. DBS is presently prescribed independently of, or even without, physical therapy even though physical therapy was a component of traditional treatment protocols before DBS was introduced, and despite findings that cortical stimulation administered during physical therapy for stroke patients increased motor performance substantially over physical therapy alone [42]. Interestingly, cortical stimulation in stroke patients has been found to cause changes in neural representation [43]. In comparison, while side effects due to DBS such as parasthesia can result, they are reversible with adjustment of stimulation or switching DBS off, implicating an absence of long-lasting changes in neural representation. An approach for DBS in PD patients analogous to combined cortical stimulation with physical therapy has not been explored despite the similar nature of the problem at hand: neurophysiologic damage resulting in motor deficit; the improvement of motor performance with physical therapy alone; the potential for neurostimulation to be used to enhance the effect of physical therapy by facilitating neuroplasticity. Studies using fMRI or transcranial magnetic stimulation (TMS) to measure changes in neural representation and cortical excitability will lead to improvements in the holisitic treatment of PD patients.
Furthermore, understanding the interaction between neural stimulation and focused exercise programs to modulate changes in the neural substrate of motor control could lead to novel methods for treating a wide range of neurological disorders. Substantial healing and recovery from brain injury often takes place by the natural mechanisms of plasticity; learning how to control plasticity, and thereby neural recovery, will open doors to greater degree of therapeutic intervention by neurostimulation. These results have far-reaching implications: plasticity might be modulated to incorporate an internal representation of an external prosthetic device. I aim to perform animal studies culminating in a clinical pilot study to test several hypotheses:
natural recovery through neuroplasticity does not occur in neurodegenerative disease (alteration of neurochemical composition) as in brain injury.
DBS will alter brain’s natural course of recovery in Parkinson’s disease.
DBS in combination with physical therapy will improve motor performance more than PT alone
DBS in combination with physical therapy will improve motor performance more than DBS alone
electrical stimulation must be paired with appropriately with physical exercise in order to create long-lasting changes in neural representation
neuroplastic changes of motor representation can be induced in the stimulated region of the brain even if that region or neighboring regions did not originally show large motor representation, but those neuroplastic changes are slower when pairing electrical stimulation of deeper structures than with comparable stimulation in the motor cortex.
Available resources and tools
My previous research investigated the information communicated in the spike activity of populations of neurons with the primary objective of applying our understanding of neural encoding to the development of medical treatment of deficits resulting from neurological disorders. Now, information can be communicated to the brain through electrical stimulation of neural tissue. Communication is a two-way process, and the most effective neural prostheses will have the capability to both listen and speak to the brain. The ability to alter pathophysiology through DBS indicates an ability to convey information to the brain. My prior experience has prepared me to conduct research at the intersection of electrophysiology, hardware, and computation. I believe by collaborating with investigators at USC’s Biomedical Simulations Resource, PET Imaging Center, and Department of Neurosurgery, and taking advantages of resources already available at USC, my research will make significant contributions to making DBS a more intelligently controlled therapy better suited for each patient. By uncovering how to control the effects of DBS, this method can replace the trial-and-error method currently used in developing DBS with an approach for controlling the effects of DBS for other indications based on neurophysioligical measurements. Collaborative work with other scientists, engineers, and neurosurgeons will also be key components to getting this research to successfully impact patient’s lives.
References
1. Schrag, A., M. Jahanshahi, and N. Quinn, What contributes to quality of life in patients with Parkinson's disease? J Neurol Neurosurg Psychiatry, 2000. 69(3): p. 308-312.
2. Herzog, J., et al., Two-year follow-up of subthalamic deep brain stimulation in Parkinson's disease. Movement Disorders, 2003. 18(11): p. 1332-1337.
3. Weaver, F., et al., Deep brain stimulation in Parkinson disease: a metaanalysis of patient outcomes. Journal of Neurosurgery, 2005. 103: p. 956-967.
4. Moro, E., et al., The impact on Parkinson’s disease of electrical parameter settings in STN stimulation. Neurology, 2002. 59: p. 706–713.
5. Dostrovsky, J.O., et al., Microstimulation-induced inhibition of neuronal firing in human globus pallidus. J Neurophysiol, 2000. 84(570-574).
6. Windels, F., N. Bruet, and A. Poupard, Effects of high frequency stimulation of subthalamic nucleus on extracellular glutamate and GABA in substantia nigra and globus pallidus in the normal rat. Eur J Neurosci, 2000. 12(11): p. 4141-4146.
7. Grill, W.M., A.N. Snyder, and S. Miocinovic, Deep brain stimulation creates an informational lesion of the stimulated nucleus. Neuroreport, 2004. 15(7): p. 1137-1140.
8. Krack, P., et al., Five-Year Follow-up of Bilateral Stimulation of the Subthalamic Nucleus in Advanced Parkinson's Disease. N Engl J Med, 2003. 349(20): p. 1925-1934.
9. Deuschl, G., et al., A Randomized Trial of Deep-Brain Stimulation for Parkinson's Disease. N Engl J Med, 2006. 355(9): p. 896-908.
10. Baltuch, G. and M. Stern, eds. Deep Brain Stimulation for Parkinson's Disease. 2007, Informa Healthcare USA, Inc.: New York.
11. Kuncel, A.M., et al., Clinical response to varying the stimulus parameters in deep brain stimulation for essential tremor. Movement Disorders, 2006. 21(11): p. 1920-1928.
12. Leblois, A., et al., Competition between Feedback Loops Underlies Normal and Pathological Dynamics in the Basal Ganglia. J. Neurosci., 2006. 26(13): p. 3567-3583.
13. Turner, R.S. and M.R. DeLong, Corticostriatal activity in primary motor cortex of the macaque. Journal of Neuroscience, 2000. 20(18): p. 7096-7108.
14. Hashimoto, T., et al., Stimulation of the subthalmic nucleus changes the firing pattern of pallidal neurons. J Neurosci, 2003. 23(5): p. 1916-1923.
15. Anderson, M., N. Postupna, and M. Ruffo, Effects of high-frequency stimualation in the internal globus pallidus on the actiivyt of thalamic neurons in the awake monkey. J Neurophysiol, 2003. 89(2): p. 1150-1160.
16. Ceballos-Baumann, A., H. Boeker, and P. Bartenstein, A positron emmission tomographic study of subthalamic nucleus stimulation in Parkinson disease: enhanced movement-related activity of motor -assocation cortex and decreased motor crotex resting activity. Arch Neurol, 1999. 56(8): p. 997-1003.
17. Sestini, S., et al., Are there adaptive changes in the human brain of patients with Parkinson's disease treated with long-term deep brain stimulation of the subthalamic nucleus? A 4-year follow-up study with regional cerebral blood flow SPECT. European Journal of Nuclear Medicine and Molecular Imaging, 2007. 34(10): p. 1646-1657.
18. Haegelen, C., et al., Does subthalamic nucleus stimulation affect the frontal limbic areas? A single-photon emission computed tomography study using a manual anatomical segmentation method. Surgical and Radiologic Anatomy, 2005. 27(5): p. 389-394.
19. Sestini, S., et al., Changes in Regional Cerebral Blood Flow Caused by Deep-Brain Stimulation of the Subthalamic Nucleus in Parkinson's Disease. J Nucl Med, 2002. 43(6): p. 725-732.
20. Nagaoka, T., et al., Changes in glucose metabolism in cerebral cortex and cerebellum correlate with tremor and rigidity control by subthalamic nucleus stimulation in Parkinson's disease: A positron emission tomography study. Neuromodulation, 2007. 10(3): p. 206-215.
21. Conca, A., et al., Effect of Chronic Repetitive Transcranial Magnetic Stimulation on Regional Cerebral Blood Flow and Regional Cerebral Glucose Uptake in Drug Treatment-Resistant Depressives. Neuropsychobiology, 2002. 45(1): p. 27-31.
22. Berney, A.M., et al., Effect on mood of subthalamic DBS for Parkinson's disease A consecutive series of 24 patients. [Miscellaneous].
23. Piasecki, S. and J. Jefferson, Psychiatric Complications of Deep Brain Stimulation for Parkinson's Disease. J Clin Psychiatry, 2004. 65: p. 845-849.
24. Hershey, T., et al., Stimulation of STN impairs aspects of cognitive control in PD. Neurology, 2004. 62(7): p. 1110-1114.
25. Trepanier, L.L., et al., Neuropsychological Outcome of GPi Pallidotomy and GPi or STN Deep Brain Stimulation in Parkinson's Disease. Brain and Cognition, 2000. 42(3): p. 324-347.
26. Chudasama, Y., C. Baunez, and T.W. Robbins, Functional disconnection of the medial prefrontal cortex and subthalamic nucleus in attentional performance: Evidence for corticosubthalamic interaction. Journal of Neuroscience, 2003. 23(13): p. 5477-5485.
27. Maurice, N., et al., Relationships between the prefrontal cortex and the basal ganglia in the rat: Physiology of the corticosubthalamic circuits. Journal of Neuroscience, 1998. 18(22): p. 9539-9546.
28. Houeto, J.L., et al., Behavioural disorders, Parkinson's disease and subthalamic stimulation. J Neurol Neurosurg Psychiatry, 2002. 72(6): p. 701-707.
29. Castelli, L., et al., Chronic Deep Brain Stimulation of the Subthalamic Nucleus for Parkinson's Disease: Effects on Cognition, Mood, Anxiety and Personality Traits. European Neurology, 2006. 55(3): p. 136-144.
30. Cassidy, M., et al., Movement-related changes in synchronization in the human basal ganglia. Brain, 2002. 125(6): p. 1235-1246.
31. Swartz, B.E., et al., The safety and efficacy of chronically implanted subdural electrodes: A prospective study. Surgical Neurology, 1996. 46(1): p. 87-93.
32. Ghika, J., et al., Portable system for quantifying motor abnormalities in parkinson’s disease. IEEE Transactions on Biomedical Engineering, 1993. 40(3): p. 276-283.
33. DeLong, M.R., Primate models of movement disorders of basal ganglia origin. Trends in Neurosciences, 1990. 13(7): p. 281-285.
34. Bergman, H., T. Wichmann, and M.R. Delong, Reversal of experimental Parkinsonism by lesions of the subthalamic nucleus. Science, 1990. 249(4975): p. 1436-1438.
35. Wichmann, T. and M.R. DeLong, Pathophysiology of Parkinson's Disease: The MPTP Primate Model of the Human Disorder. Annals of the New York Academy of Sciences, 2003. 991(1): p. 199-213.
36. Kuhn, A.A., et al., Event-related beta desynchronization in human subthalamic nucleus correlates with motor performance. Brain, 2004. 127(4): p. 735-746.
37. Hutchison, W.D., et al., Neuronal oscillations in the basal ganglia and movement disorders: Evidence from whole animal and human recordings. Journal of Neuroscience, 2004. 24(42): p. 9240-9243.
38. Hammond, C., H. Bergman, and P. Brown, Pathological synchronization in Parkinson's disease: networks, models and treatments. Trends in Neurosciences, 2007. 30(7): p. 357-364.
39. Feng, X., et al., Toward Closed-Loop Optimization of Deep Brain Stimulation for Parkinson's Disease: Concepts and Lessons from a Computational Model. Journal of Neural Engineering, 2007. 4: p. L14-L21.
40. Marmarelis, V.Z. and T.W. Berger, General methodology for nonlinear modeling of neural systems with Poisson point-process inputs. Mathematical Biosciences, 2005. 196(1): p. 1-13.
41. Song, D., et al., Nonlinear Dynamic Modeling of Spike Train Transformations for Hippocampal-Cortical Prostheses. IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, 2007. 54(6): p. 1053-1066.
42. Teskey, G., C. Flynn, and C. Goertzen, Cortical stimulation improves skilled forelimb use followinga focal ischemic infarct in the rat Neurol Res 2003. 25: p. 794 –800.
43. Adkins-Muir, D. and T. Jones, Cortical electrical stimulation combined with rehabilitative training: Enhanced functional recovery and dendritic plasticity following focal cortical ischemia in rate. . Neurol. Res., 2003. 25 p. 780-788.